

History
Honoring Our Past. Envisioning Our Future.
New York Eye and Ear Infirmary of Mount Sinai (NYEE) proudly celebrates its 200-year anniversary as America’s first specialty hospital founded in 1820. Originally established as a charitable institution to provide care for New York City’s poor with diseases of the eyes, ears, nose, and throat, the Infirmary quickly grew its reputation as one of the leading centers for innovative clinical care, patient research, and medical education. By 1918, NYEE had already treated over one million patients and established leading residency programs in ophthalmology and otolaryngology (ENT).
Today, NYEE remains at the forefront for innovative surgical specialty services. The institution serves as the clinical site for breakthrough translational research—introducing many novel diagnostic and surgical techniques—with a growing network of satellite practices across the New York metropolitan area. As NYEE looks forward to its third century of specialty care, the Infirmary remains committed to its founding mission of serving the community, as well as patients nationally and internationally.
NYEE History Book
Let our coffee table book take you on a journey through the 200-year history of NYEE. Get to know the people and events that shaped our celebrated specialty hospital and learn about our lasting impact on the fields of ophthalmology and otolaryngology. Learn More
America’s First Black Ophthalmology Specialist
Celebrate the incredible life and legacy of Dr. David Kearny McDonogh. A former slave, he served on NYEE staff as America’s first Black ophthalmology specialist. Learn More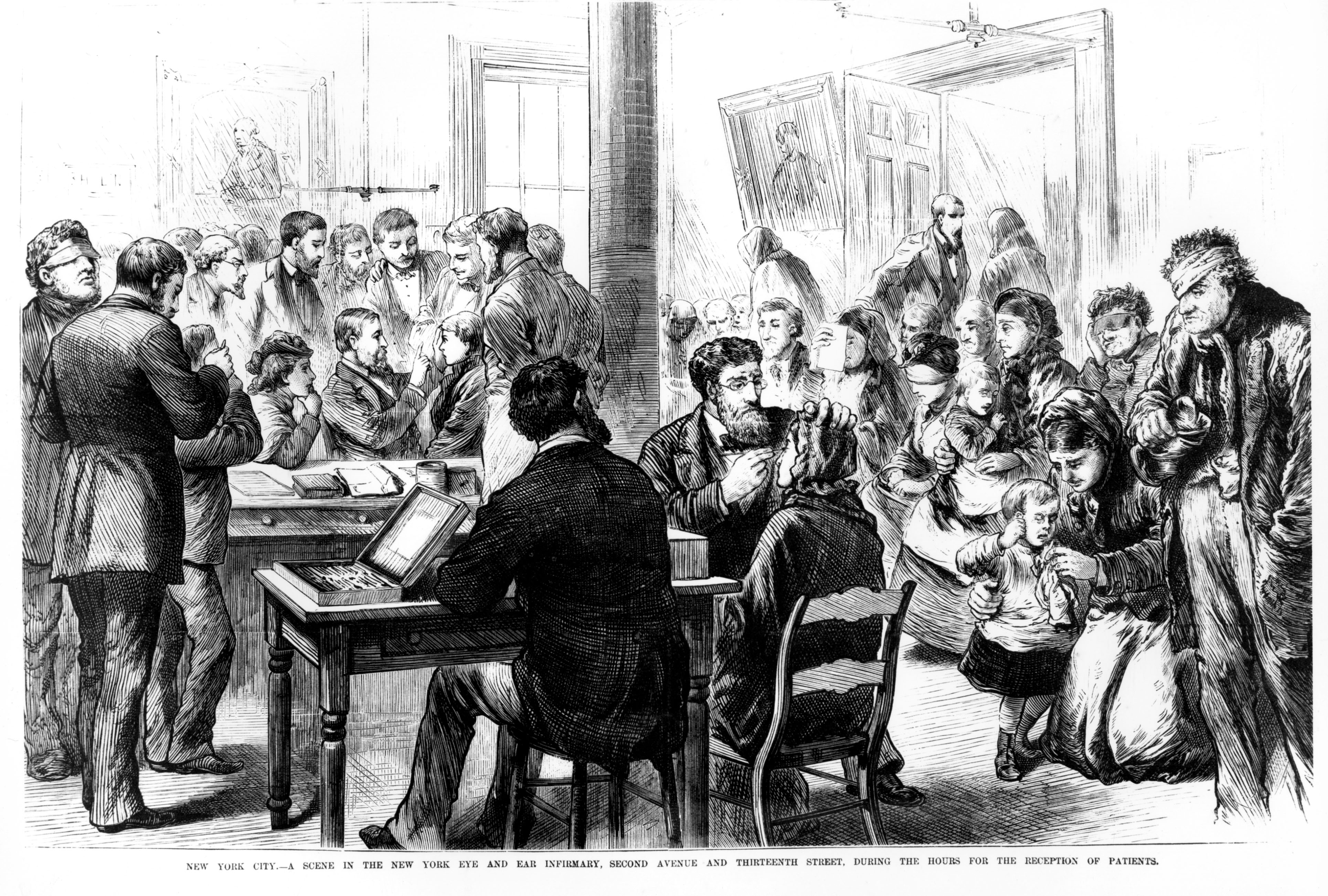
Historic Timeline of NYEE
Discover the fascinating history of America’s oldest specialty hospital through our digital history timeline. Learn More